Massage for Chronic Neck Pain: How Many Sessions, What It Costs, and When to Quit
Intro / Hook
The real question isn't whether massage helps a stiff, aching neck. It's whether it will help yours, and how much it'll cost you to find out. That's the question that walks through our door, and most articles dodge it — they tell you massage "promotes relaxation" and "may relieve tension" and leave you to guess at the rest.
So here's the honest version. Massage works for chronic neck pain. The research backs it. But it works the way a prescription works, not the way a cure works — it's a dose, not a fix. Get the dose right and the relief is real. Get it wrong, or treat it as a one-time miracle, and you'll spend money on something that was never going to stick.
This piece answers the questions the dodgy ones skip. How many sessions it actually takes. What a real course costs. Why the relief fades, and how fast. What you can do between visits — and for free — to make it last. We treat necks for a living, so the protocols here are the ones we use. The numbers all come from the clinical trials, not the marketing.
Does It Work?
Yes — for pain, in the short term. That's the verdict the evidence actually supports, stated plainly.
First, what chronic neck pain even means here, since most articles never say it: ordinary neck pain that's stuck around for at least three months — the everyday mechanical kind, with no specific injury or structural cause behind it. That's exactly the population the research below studied, and it describes most of the necks that ache from desks, phones, and stress. Pain from a recent injury, or pain that shoots down your arm, is a different problem with different rules — that's the red-flags section near the end, not this.
The strongest summary comes from a meta-analysis that pooled 13 studies on neck pain: massage produced a significant reduction in pain intensity, with a standardized mean difference of 0.49 (95% CI 0.07–0.92, P=0.02). The NIH's own center for complementary health agrees — massage "may be helpful for neck or shoulder pain, but the benefits may only last for a short time" (NCCIH). Short-lived, but real.
Two wins are worth pulling out, because they cut against the "it's just a luxury rub" assumption.
First, massage beats doing the reading yourself. In a trial that pitted hands-on massage against a self-care book for neck pain, the massage group's neck function improved 39% against the book's 14% — a relative risk of 2.7 in massage's favor at ten weeks (Sherman 2009). Information is cheap and useful. Skilled hands on the muscle did more.
Second, people lean less on painkillers. In a related trial on back pain, the massage group used the least medication of any group and had the lowest follow-up care costs (Cherkin 2001, P<.05). That's back-pain data, not neck — we're not going to pretend otherwise — but it points in a direction worth knowing: relief you can feel tends to reduce what you reach for in the cabinet.
Now the part most clinics won't tell you — and where the kind of massage matters. That meta-analysis tested passive massage in isolation: soft-tissue work, Swedish technique, myofascial release, nothing layered on top. On that alone, it found no significant effect on disability or range of motion. A passive rub, however good it feels, doesn't by itself give you back how far you can turn your head.
But passive soft-tissue work isn't the whole toolkit — and that's the distinction most articles miss. When a therapist adds assisted contract-relax stretching — you contract a muscle gently against our resistance, then we ease the joint into a little more range — cervical range of motion does improve. Two related-but-distinct methods do this, and they're worth telling apart: muscle energy technique (MET), the gentle, low-force approach with roots in osteopathic medicine, and PNF, a stronger-effort cousin out of physical-therapy rehab. They share the same contract-then-stretch logic but aren't the same technique. A systematic review of 21 trials found muscle energy technique "improves cervical range of motion in patients with chronic neck pain," best when paired with rehab (Sbardella 2021), and a randomized trial found that adding stretching to hands-on care improved range in extension, rotation, and side-bending (Alfawaz 2020). That evidence is promising rather than airtight — the trials are small and vary in quality — and the gain is specifically in movement, not extra pain relief.
So the honest bottom line: a passive massage is for pain. Getting range of motion back is the job of the active, assisted techniques layered on top — which is exactly how we work, and exactly why how your therapist treats you matters more than whether you simply "got a massage."
The Dose
If you take one thing from this article, take this: with massage, dose is the lever. Not the technique, not the spa, not the playlist. How long and how often.
The cleanest evidence is a dosing trial out of the University of Washington group — 228 adults with nonspecific chronic neck pain, randomized across five different massage "doses" or a no-treatment wait-list — a comparison group that got no massage at all during the four-week study (and were given a course of their own afterward) (Sherman 2014, Annals of Family Medicine). They measured who hit a clinically meaningful improvement in neck disability after four weeks. The results sort cleanly by dose.
It's worth knowing how that trial was actually run, because these are exactly the questions a good therapist asks. It excluded specific diagnoses — pinched nerves (radiculopathy), recent accidents, fractures, anything with an identifiable structural cause — so the numbers describe ordinary mechanical neck pain, not nerve or injury pain. Treatment was a structured protocol, not a freestyle rub: eight licensed massage therapists with five-plus years of experience each, trained to follow the same sequence — assess range of motion, work the neck directly, release the muscles compensating around it, then integrate — while drawing on a broad hands-on toolkit (gliding and kneading, trigger-point, myofascial, and assisted stretching), per the published trial protocol. And the 30- versus 60-minute sessions worked the same regions — the neck and the muscles that feed it — so the gap between them was time and dose, not a different part of the body.
Sixty-minute sessions, three times a week, made people about five times as likely to reach a meaningful improvement in neck function as getting no treatment at all (adjusted relative risk 4.98). Read that precisely, because it's easy to mangle: it's roughly 5× the likelihood of meaningful improvement versus no treatment — not "five times better than one session a week," and not "five times less pain." Two 60-minute sessions a week came in around 3.4×. For pain intensity specifically, the multiplier was smaller — about 2.7× for the top dose.
And here's the line that separates a working course from wasted money: the 30-minute sessions didn't beat the wait-list at any frequency. Half-hour appointments, twice or three times a week, performed no better than doing nothing. Only the 60-minute sessions, two to three times a week, moved the needle. The trial even put a number on the slope — each additional 60-minute session per week was worth roughly 1.8 points of improvement on the neck disability index.
So the booking that actually works isn't "a massage." It's a 60-minute session, two to three times a week, for about a month. Anything shorter and you're paying for relaxation, not results.
The Cost Math
This is where the honest version pays off, because once you know the working dose, you can do the math nobody does for you.
A clinically effective course is roughly 8 to 12 sixty-minute sessions over about four weeks — two to three a week, per the dosing trial. At our $99 new-client rate for a 60-minute therapeutic massage, here's what that first month actually looks like:
Dose-and-cost decision table
| What you book | Sessions over ~4 weeks | Cost at $99/session | What the evidence says |
|---|---|---|---|
| 60 min, 1×/week | ~4 | ~$396 | Below the effective threshold (RR not significant). |
| 60 min, 2×/week | 8 | ~$792 | Works (~3.4× likelihood of meaningful improvement). |
| 60 min, 3×/week | 12 | ~$1,188 | Best supported (~5× likelihood vs. no treatment). |
$99 is our new-client rate for your first 60-minute therapeutic massage — the simplest way to start a course. Ongoing sessions are at our standard rate; ask us about package pricing for a full four-week course.
The table makes the trap obvious. The once-a-week habit most people default to sits below the threshold the evidence supports — and as we saw, shorter 30-minute sessions don't beat no treatment at any frequency, so trimming there just sets money on fire. If you're going to spend, spend on the dose that has a result attached to it.
Think of it the way we think about any leak: fix the leak before you keep filling the bucket. A proper four-week course is a defined cost with a defined goal — get the pain down, then decide what's worth maintaining. Drifting in for a 60-minute session whenever your neck flares up is the slow drip that adds up to more than the course and delivers less. Decide on a course, run it, measure your own neck against it. That's the spend that earns its keep. Book a course of sessions with us.
Why Relief Fades
Here's the part that sets up everything after it: the relief doesn't hold on its own.
The same research group followed people past the initial course. After four weeks of massage, they re-randomized participants — some got six more weekly "booster" sessions, some stopped (Cook 2015, The Spine Journal). At 12 weeks, the boosters were still paying off: the extra-massage group held a significant advantage in neck disability (adjusted relative risk 1.56, P=0.018). Keep treating, keep the benefit.
Then they stopped. By 26 weeks, with treatment over, the advantage had faded to nothing statistically meaningful — disability RR slipped to 1.22 (P=0.277), pain RR to 1.09 (P=0.558). The authors' own conclusion: the benefits "diminished and were no longer statistically significant several months after the treatments stopped."
That's not a knock on massage. It's the truth about it. Massage relieves pain while you're doing it and for a while after, and more of it extends the benefit — but as your only lever, it drains back down within a few months of the last appointment. Which means the real question isn't just "does massage work." It's "what do I do between sessions so I'm not buying the same relief over and over." That's the next move.
Make It Last
We'll be straight about this up front: no head-to-head trial has tested "massage plus an anti-inflammatory lifestyle" against "massage alone" for neck pain. Anyone who tells you the combination is proven is guessing. What we have is converging mechanism — and years of watching it play out in our own clients. The relief lasts longer in the people who change what's happening between sessions — not only what happens on the table. Here's the part that's actually evidenced.
Omega-3s lower the inflammatory load. A 2025 meta-analysis of 41 randomized trials found omega-3 supplementation produced a moderate, meaningful reduction in chronic pain intensity — a standardized mean difference of −0.55 (Frontiers in Medicine 2025). Two honest caveats. It helped rheumatoid arthritis and migraine clearly; it did not help osteoarthritis. And it's broad inflammatory and chronic pain, not neck pain isolated as its own subgroup. Notably, the lower doses worked best — at or under 1.35 grams a day, more wasn't better.
Less sugar lowers a key inflammation marker. In a controlled trial, just three weeks of low-to-moderate sugar-sweetened drinks raised hs-CRP — a standard marker of systemic inflammation — by 60 to 109% in healthy young men (Aeberli 2011). That's a fast, measurable swing from sugar alone. Cutting back plausibly lowers the inflammatory load the massage is working against. The direct "sugar causes neck pain" study doesn't exist — but the inflammation link is solid and the move is free.
Hydration supports the tissue itself. This one is mechanism, not a pain trial, and we'll label it that way. Your spinal discs are mostly water, and their ability to cushion load depends on staying hydrated — disc stiffness and mechanics shift with hydration state (J Biomech Eng 2015). Drinking enough water won't cure a bad neck, but it supports the structures everything else is trying to help.
None of these is a substitute for the dose. They're the thing that keeps the dose from draining away. Massage knocks the pain down; lower inflammation and well-supported tissue are what let it stay down longer between visits. Mechanism, not a guarantee — but it's sound, it's low-risk, and we see the difference.
The DIY Branch: Know Your Neck
If the cost math points you toward doing more yourself between sessions — and for a lot of people it should — you need to know what you're actually working on. Most self-massage advice has you rubbing the spot that hurts, which is often not where the problem lives. Five muscle groups do most of the work in a chronically tight neck.
Suboccipitals — the small, deep muscles where the skull meets the spine. They're the classic source of the tension headache that wraps from the base of the skull around toward the eyes (PainScience on suboccipital trigger points). Tight here, and your head feels heavy and your eyes ache.
Upper trapezius — the big sloping muscle from the base of the neck to the shoulder. This is the "I carry my stress in my shoulders" muscle. It hauls your shoulder up toward your ear all day at a desk.
Levator scapulae — runs from the upper neck down to the inside corner of the shoulder blade. The sharp, pinpoint ache where neck meets shoulder is usually this one. It hates long static postures.
Sternocleidomastoid (SCM) — the rope-like muscle on the front-side of your neck that you can feel when you turn your head. Overlooked because it's on the front, but a major player in headaches and that "can't turn my head" stiffness.
Scalenes — deep on the side of the neck, beneath the SCM. They can refer pain into the chest, shoulder, and even down the arm, which is why side-of-neck tension sometimes shows up far from the neck.
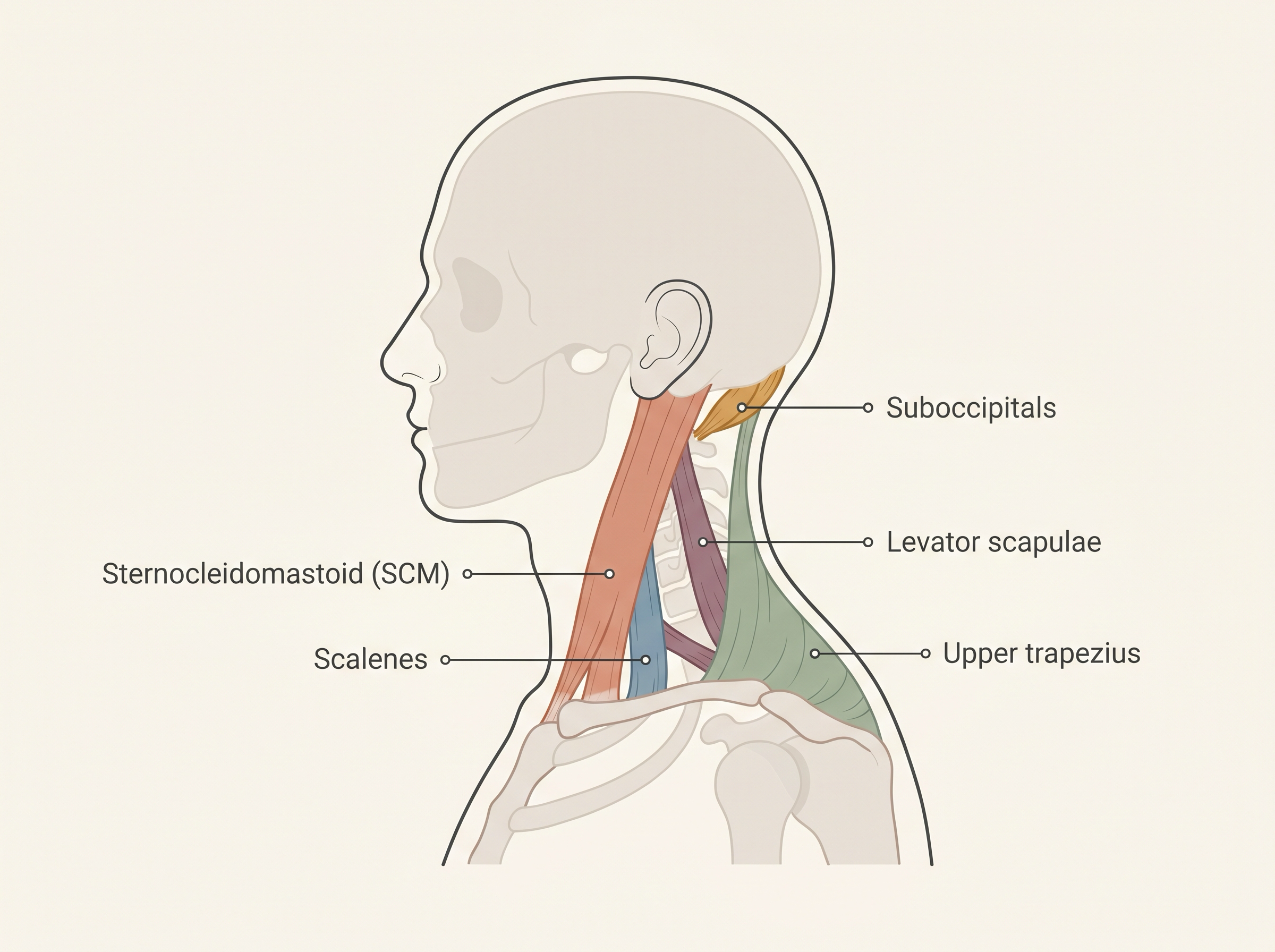
The five muscles that drive most chronic neck tension — and where each one actually sits.
One thing to hold onto from the last section: working these muscles yourself is for tension and pain relief between sessions. Restoring range of motion is the job of the assisted-stretching and muscle-energy work we do in the clinic — self-massage keeps you looser between visits, but it doesn't replace that. We won't pretend otherwise. Work with one of our therapists.
Self-Massage Protocol
Here's a simple routine tied to the muscles above. Five to ten minutes, a few times a week. No tools required — your hands are enough, though a tennis ball or a small massage ball makes the deep work easier. Slow and steady beats hard and fast every time.
Start away from the neck itself. The counterintuitive move: begin on the upper traps and the shoulders, not the painful neck. Knead the meat of the shoulder between your fingers and the heel of your opposite hand for a minute or two per side. Loosening the big muscles first means the small, irritable ones aren't fighting you when you get there.
Suboccipitals — the base of the skull. Tilt your head back into your fingertips (or a ball against a wall) right where the skull meets the neck. Small, slow circles. Let the weight of your head do the pressing. Thirty to sixty seconds. This is the one that quiets a tension headache.
Levator scapulae — the corner. Find the tender spot where your neck meets the top of your shoulder blade. Press and hold with steady pressure, breathe, and slowly turn your head away to add a gentle stretch. Hold, don't grind.
SCM — gently, on the front. Pinch the rope-like muscle on the side-front of your neck lightly between thumb and finger and roll it. Light pressure only here — this is a sensitive area, and there's no prize for going hard.
That last point is the rule for all of it: gentle and consistent does more than aggressive and occasional. If a spot is sharp, sends tingling down your arm, or makes you dizzy, stop. That's not a knot to push through — and the next section explains why.
Red Flags: When to See a Doctor, Not a Therapist
Most neck pain is muscular and safe to work on. Some isn't, and the difference matters. Massage — DIY or professional — is the wrong move for the following, and a couple of them are genuine emergencies.
Stop and see a doctor if you have:
- Burning, tingling, numbness, or weakness running into the arm or hand. That's a nerve signal, not a muscle knot, and pressing on it can make things worse (spine-health).
- Neck pain after a recent accident, fall, or trauma. Rule out structural injury before anyone touches it.
- A new, severe headache unlike your usual ones, especially with a stiff neck and fever — that combination needs urgent assessment (Mayo Clinic).
- Neck pain with fever, unexplained weight loss, or pain that's worse at night — systemic warning signs that aren't a job for the massage table.
And the one nobody mentions: don't let anyone crank hard on the front or sides of your neck. Aggressive pressure or forceful manipulation near the vertebral arteries — the vessels running up through the neck to the brain — has, in rare cases, caused arterial injury and stroke. This is exactly why our self-massage rule is gentle, and why "no pain, no gain" has no place on a neck. If a treatment hurts in a way that feels wrong, it's wrong.
When in doubt, get it looked at. A good therapist will refer you out for any of the above without hesitation — that's part of the job too.
Conclusion
Massage earns its place in chronic neck pain treatment — but only when you treat it like what the evidence says it is. A measured dose: 60-minute sessions, two to three times a week, for about a month. Expect real short-term relief on pain, not a cure for your range of motion. Expect that relief to fade within a few months if massage is your only lever — so pair it with the cheap stuff that lowers your inflammatory load and supports the tissue, and learn to work your own neck between visits.
Fix the leak before you keep filling the bucket. Book the dose that has a result attached to it, run the course, and measure your own neck against it. If you want help getting the protocol right — or you're not sure your neck is safe to work on — talk to us first.